

June 3, 2026, Alexandria, VA The American Thyroid Association® (ATA®) annually recognizes clinicians, academicians, and…
Read More
June 3, 2026, Alexandria, VA The American Thyroid Association® (ATA®) annually recognizes clinicians, academicians, and…
From Clinical Thyroidology® for the Public: The FDA has warned against using the weight loss…
Drs Kaniksha Desai and Jacqueline Jonklaas discuss medications and the thyroid gland. Medications are frequently…
From Clinical Thyroidology® for the Public: Bariatric surgery is generally safe, but problems after the…

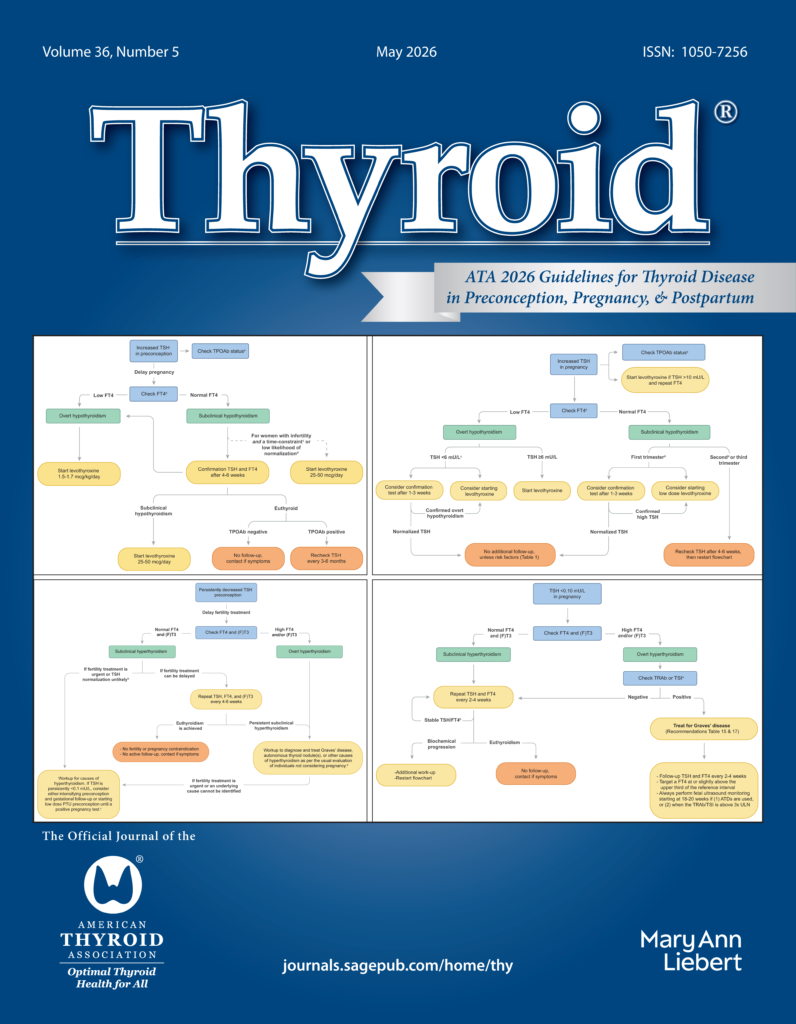
Thyroid Hormone Synthesis Without Thyroglobulin C. Young, X. Zhang, A.P. Kellogg, T.L. Fonseca, K. Pena,…
© 2026 American Thyroid Association.



